
History taking & The Med Den Method
Contents
The Calgary-Cambridge framework
The Med Den system
How The Med Den System Fits Into The Consultation
A Note on SOCRATES & introducing ‘OTAPS’
Management Comes From Diagnosis
The Key Takeaway
The Calgary-Cambridge Framework
One of the most common questions medical students ask is:
"Where does The Med Den system fit into the history taking process?"
The answer is simple.
It fits within the information gathering stage of the consultation.
Most medical schools teach a structured consultation model such as the Calgary-Cambridge framework. This framework helps ensure that consultations are patient-centred, organised, and safe.
Basic Calgary-Cambridge Model by Kurtz and Silverman in 1996 ; link to image
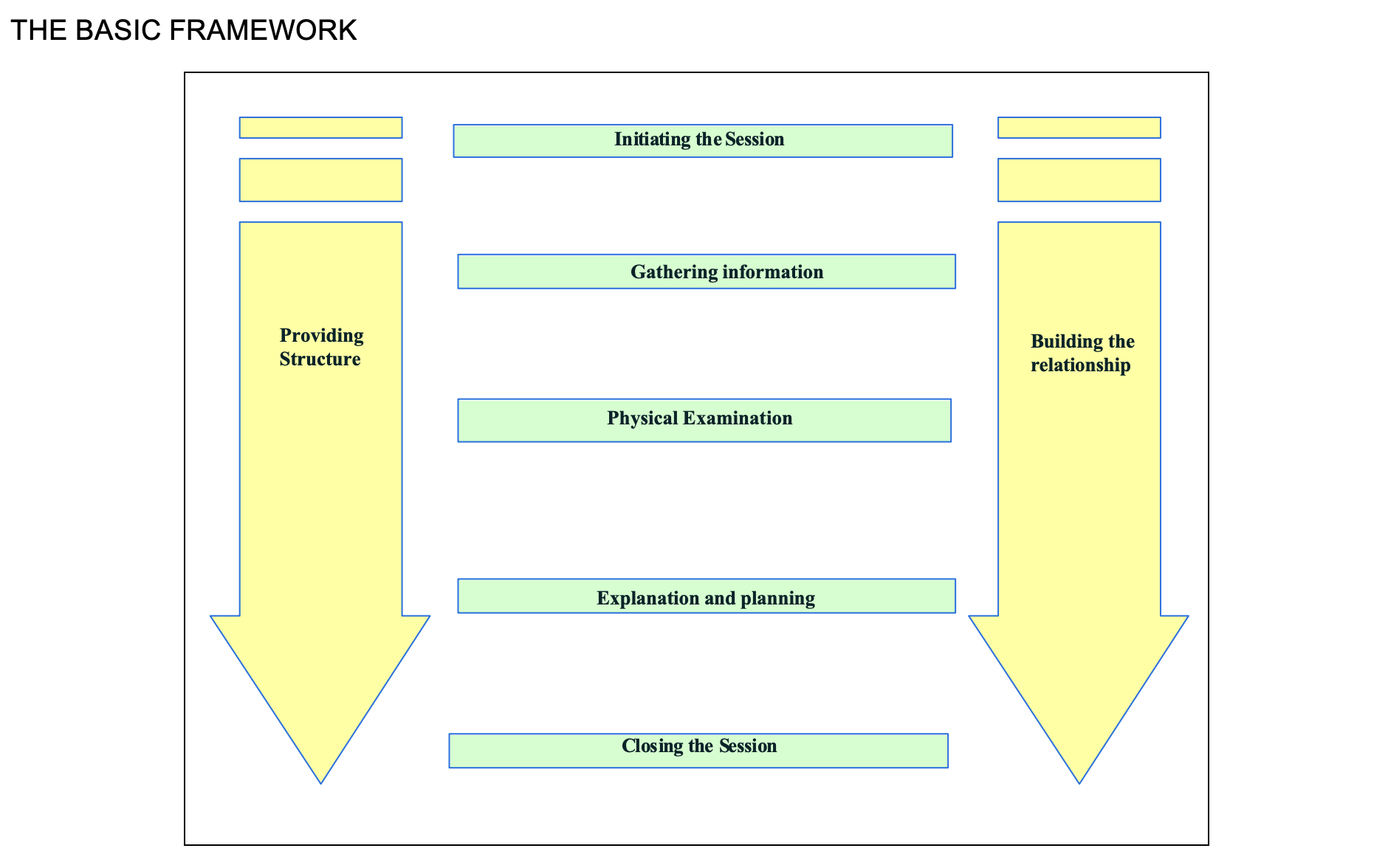
The Med Den system does not replace Calgary-Cambridge. Instead, it helps answer the most important question during the information gathering phase:
"What is going on with this patient?"
Many students learn these stages well but struggle with what to think about whilst gathering information.
This is where The Med Den system helps.
The Med Den System
Whenever a patient presents with a symptom, ask yourself four questions:
1. What is the patient actually saying?
Before jumping to diagnoses, define the symptom.
Patients often use words differently from clinicians.
For example:
"Dizziness" may mean vertigo, light-headedness, imbalance, or pre-syncope.
"Chest pain" could be pain, pressure, tightness, burning, or discomfort.
"Weakness" may represent fatigue, breathlessness, pain, or true loss of power.
A diagnosis cannot be made until the presenting complaint is clearly defined.
2. What is the worst thing this could be?
Every symptom has diagnoses that cannot be missed.
Examples include:
Chest pain → Acute coronary syndrome
Headache → Subarachnoid haemorrhage
Back pain → Cauda equina syndrome
Shortness of breath → Pulmonary embolism
These diagnoses guide your red flag questions.
3. What is common?
Medicine is often about balancing risk with probability.
While dangerous diagnoses must be considered, common conditions remain common.
For chest pain this might include:
Musculoskeletal chest pain
Gastro-oesophageal reflux disease
Anxiety-related symptoms
For headache this might include:
Tension headache
Migraine
Your history should help distinguish common conditions from serious alternatives.
4. What investigation or finding would change my differential diagnosis list?
As information is gathered, ask:
"What piece of information would move a diagnosis up or down my list?"
Examples:
For chest pain:
ECG changes
Raised troponin
Pain reproducible on palpation
For shortness of breath:
Oxygen saturations
Peak flow
Chest X-ray findings
For abdominal pain:
Urine dip
Pregnancy test
Blood tests
This question helps focus your history, examination, and investigations.
How The Med Den System Fits Into The Consultation
The Med Den system sits primarily within the gathering information and physical examination stages of the consultation.
It helps you:
Define the symptom
Generate differential diagnoses
Identify red flags
Ask focused questions
Select appropriate examinations
Choose useful investigations
Once enough information has been gathered, you move into the next stage of the consultation.
A Note on SOCRATES & introducing ‘OTAPS’
SOCRATES is an excellent tool for assessing pain. However, one of the most common mistakes medical students make is trying to force it onto every presentation.
Many symptoms are not pain-related. For example:
Fatigue
Weight loss
Dizziness
Low mood
Breathlessness
Falls
For these presentations, SOCRATES can feel unnatural and often misses important information.
Over time, I have found the following framework useful for almost any symptom presentation:
OTAPS
O: Onset
When did the symptom begin?
Consider:
Sudden or gradual onset?
Has it remained stable, improved, or worsened?
Was there a triggering event?
T: Timing
When does the symptom occur?
Consider:
Constant or intermittent?
Worse at a particular time of day?
Any cyclical or recurring pattern?
A: Associated Symptoms
What else is happening?
This is where your differential diagnoses begin to guide your questioning.
For example:
Chest pain → breathlessness, palpitations, nausea
Headache → visual symptoms, vomiting, neurological symptoms
Fatigue → weight loss, fevers, night sweats
P: Provoking or Palliating Factors
What makes the symptom worse or better?
This often provides important diagnostic clues and can help distinguish between competing diagnoses.
S: Severity
How much is this affecting the patient's life?
Consider the impact on:
Work
Home life
Exercise
Sleep
Relationships
Remember, severity is not simply a numerical score. It is about understanding the functional impact of the symptom.
Why OTAPS Matters
OTAPS is not intended to replace clinical reasoning.
Instead, it provides a simple structure that helps gather the key information required for most presentations before moving on to more condition-specific questions.
Combined with The Med Den approach of:
Defining the symptom
Considering the worst-case diagnosis
Considering the common diagnoses
Identifying the investigations or findings that would change your differential diagnosis
OTAPS provides a practical framework for gathering information efficiently and systematically.
Management Comes From Diagnosis
Many students focus heavily on management plans.
However, management is usually the easy part.
The difficult part is working out what is going on.
If your diagnosis is correct, management often follows naturally.
For example:
Asthma diagnosed → Asthma treatment pathway
Pneumonia diagnosed → Antibiotic pathway
Acute coronary syndrome diagnosed → Emergency referral pathway
This is why The Med Den focuses on clinical reasoning rather than memorising management plans.
The Key Takeaway
The Med Den system is not another history-taking structure.
It is a clinical reasoning framework that sits inside the information gathering stage of the consultation.
While Calgary-Cambridge tells you how to conduct a consultation, The Med Den helps you think about what might be causing the patient's symptoms.
In simple terms:
Calgary-Cambridge teaches you how to ask questions.
The Med Den teaches you why you are asking them.
Happy learning,
Dr Shabir